Dr. Theo Vance
Exhibit A · Portrait
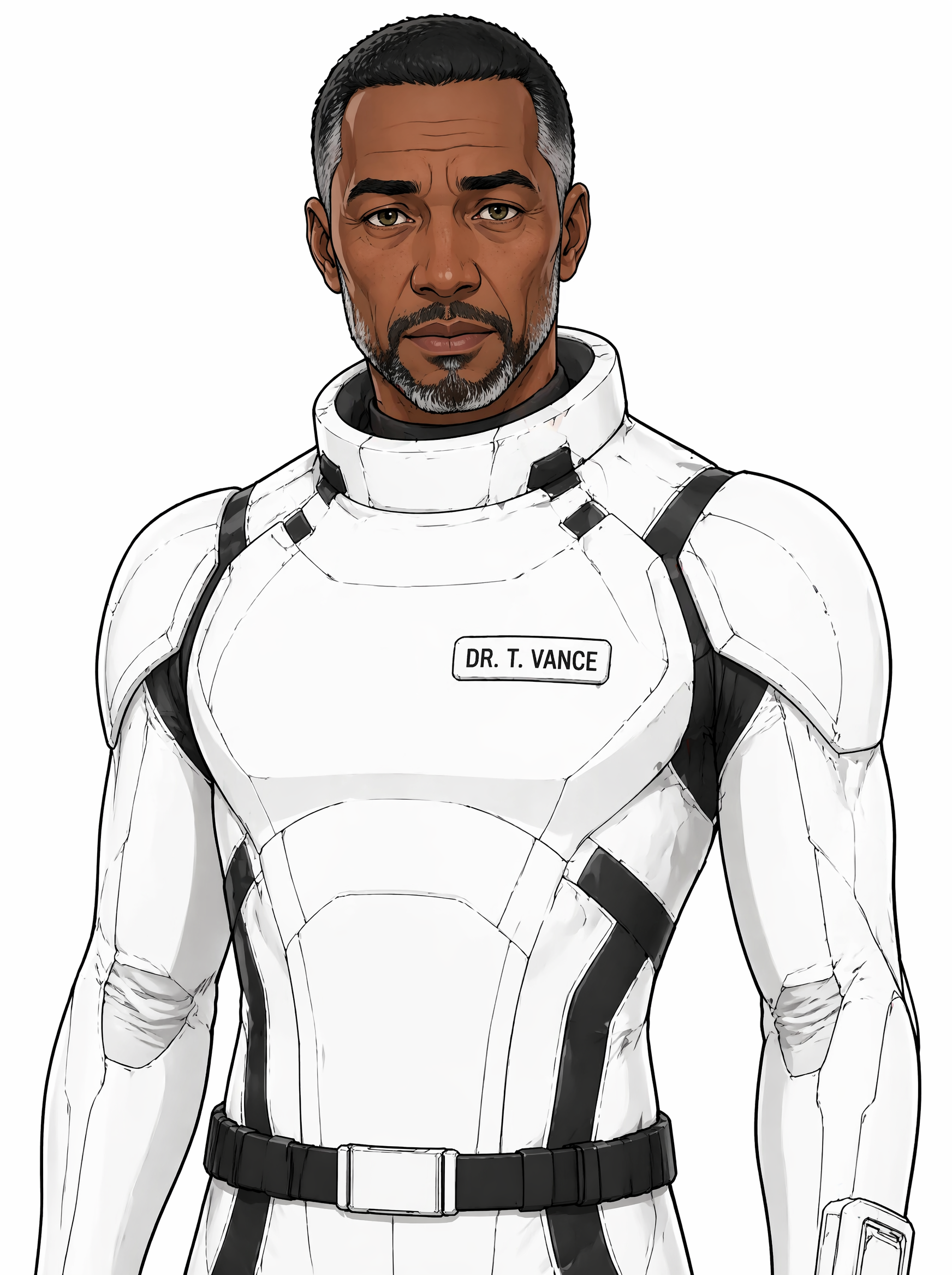
Exhibit B · Closeup
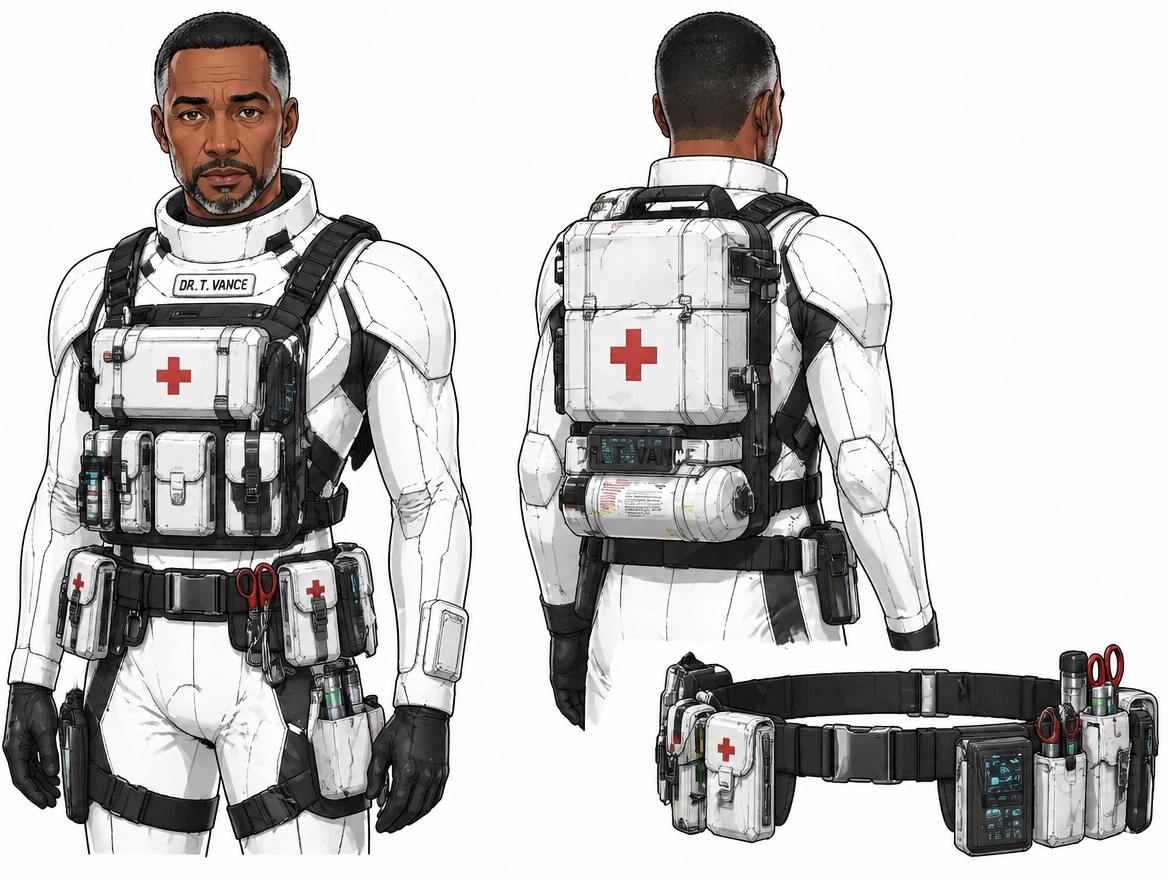
Exhibit C · Physique
Exhibit D · Candid record
- Height
- 183 cm
- Build
- lean, long-limbed
- Posture
- slightly stooped from years over surgical tables
- Gait
- pending
- Hair
- short-cropped black with salt at the temples
- Eyes
- warm brown with green flecks, kind but tired
- Skin
- deep warm brown
- Distinguishing
- reading glasses he never remembers are pushed onto his head; small silver pendant of undefined faith
- Callsigns
- Dr. Theo Vance, Dr. Vance, Vance
- Origin
- Earth (refugee corridors)
- Heritage
- Ethiopian and English
- Born
- 1979-07-08 · age 46
Operational profile
- Composure
- Acumen
- Empathy
- Endurance
- Authority
Environmental tolerance
- Vacuumnominal
- Radiationnominal
- Thermalnominal
- G-Loadnominal
Skills (top 3)
- Trauma medicine
- field-hospital surgery under sustained crisis
- Crew psychiatric monitoring
- remembers what each crew member eats and who is due to crack
- Stress-load absorption
- carries others' breakdowns until his own arrives
Decision profile
- Risk tolerancecautious / aggressive
- Cooperation leansolo / ensemble
- Disclosure leandiscrete / declarative
- Tempodeliberate / instinctive
Alignment & faction
- Order / improvisation rule-keeper / rule-breaker
- Primary
- ADN-1 Crew
- Secondary
- Crisis-period medical corps (former)
Failure-mode flags
- invisible breaking-point risk
- absorbed-stress collapse
RESTRICTED // PSYCHOLOGICAL ASSESSMENT // PRE-PRODUCTION CANON
Day-to-day: Vance. Formal: Dr. Vance.
Function
Psychological stabilizer. Makes long runs survivable.
Backstory
Trauma surgeon in collapsed-infrastructure zones. Ran a field hospital through two evacuation campaigns. Watched three colleagues burn out, did not. Stays because the work stays.
Gift
Keeps people alive, physically and psychologically. Absorbs stress that would break others. The crew will break and he is the reason it reforms.
Reason for yes
The call came while he was on shift. He finished the shift first. Said yes on the drive home because the question was worse than the answer.
Personality
Observant, steady, the one who remembers what everyone eats and who is due to crack. Listens more than speaks. Carries the crew’s exhaustion so they do not have to.
Shadow
Absorbs so much that his own breaking point is invisible until it arrives.
Visual register
Warm terracotta dominant, copper accent (on stethoscope, pendant chain). Tall (183 cm), lean and long-limbed, slightly stooped from years over surgical tables. Short-cropped black hair with salt at the temples; warm brown eyes with green flecks, kind but tired; deep warm brown skin. Reading glasses he never remembers are pushed up onto his head; small silver pendant of undefined faith. Off duty: white medical tunic over ship-grays, stethoscope slung, medical satchel close at hand. Recurring gesture: places a hand briefly on the shoulders of patients, and of crew members who do not yet know they are patients. Voice is warm low-mid male, soft-spoken, pauses before answering; accent present but placeable only by those familiar with it.
Recurring object
A pocket-sized leather medical notebook, scrawled with handwriting in three alphabets, bent to fit his coat pocket.
THRESHOLD INTERNAL // SELECTION PROGRAM // EYES-ONLY
Sources of evidence
- Surgical service record, two evacuation campaigns (2071 to 2074, 2075 to 2077)
- Patient outcome statistics, blinded sample (n = 2,418)
- Three colleague depositions, voluntary
- Personal medical journal, partial (consented for review through page 42)
- Field-hospital incident report, [REDACTED]
Operational assessment
Subject is a trauma surgeon with a documented capacity to operate at full effectiveness for shifts measured in days. His patient outcome statistics across two evacuation campaigns are top-decile and remain so even when adjusted for triage volume. He has stayed in active field practice past the age at which his peers transitioned to administrative roles. Subject's strongest competency is not surgical technique, which is excellent but not unique, but his ability to keep ambulatory crew functioning at distance from medical support.
Psychological profile
Subject demonstrates absorbed empathy at clinical levels. He remembers what patients eat and who is due to crack, including patients who have not yet declared themselves as such. Affective register is warm low and resourced; the resourcing is the flag, not the warmth. The analyst's read is that subject's calm is paid for daily and the bill is not visible in his behavior until it is no longer payable.
Risk factors
- Invisible breaking point. Subject's coping is internal and well-defended, which means the moment of failure will arrive without warning the rest of the crew. Long missions require co-monitoring.
- Absorbed-stress collapse. Subject carries others' breakdowns until his own arrives. A nine-month sealed transit will accumulate against him faster than a field-hospital cycle.
- Subject does not say no. He will accept duty rotations beyond his capacity. Mission medical scheduling must enforce limits without his consent.
Recommendation
ADVANCE to Phase 4 evaluation. Pair with on-vessel co-monitoring protocol; consider Hale candidacy as buffer.
Counter-evidence to consider
Selecting the strongest sustaining medical figure on the program's books places the entire crew's medical safety on a single point of failure. Reviewers should determine whether a backup medical role can be carried by a non-medical crew member with augmented training before signing this recommendation.